CXR findings are that of a small lung with ipsilateral mediastinal shift, and in one third of cases the anomalous draining vein may be seen as a tubular structure paralleling the right heart border in the shape of a Turkish sword (“scimitar”).
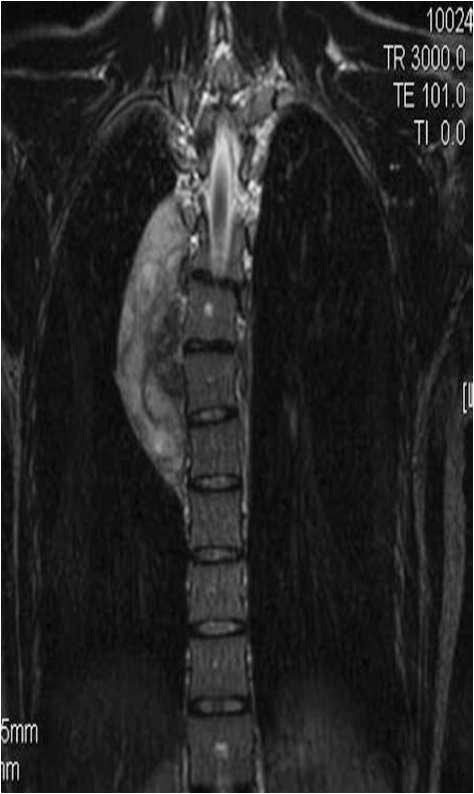
Scimitar syndrome is associated with congenital heart disease, ipsilateral diaphragmatic anomalies and vertebral anomalies